Insomnia
| Insomnia | |
|---|---|
| Classification and external resources | |
| ICD-10 | F51.0, G47.0 |
| ICD-9 | 307.42, 307.41, 327.0, 780.51, 780.52 |
| DiseasesDB | 26877 |
| eMedicine | med/2698 |
| MeSH | D007319 |
Insomnia is a symptom[1] that can accompany several sleep, medical and psychiatric disorders, characterized by persistent difficulty falling asleep and/or difficulty staying asleep. Insomnia is typically followed by functional impairment while awake.
Both organic and non-organic insomnia without other cause constitute a sleep disorder, primary insomnia.[2] One definition of insomnia is "difficulties initiating and/or maintaining sleep, or nonrestorative sleep, associated with impairments of daytime functioning or marked distress for more than 1 month."[3]
According to the United States Department of Health and Human Services in the year 2007, approximately 64 million Americans regularly suffer from insomnia each year.[4] Insomnia is 41% more common in women than in men.[5]
Contents |
Classification
Types of insomnia
Although there are several different degrees of insomnia, three types of insomnia have been clearly identified: transient, acute, and chronic.
- Transient insomnia lasts for less than a week. It can be caused by another disorder, by changes in the sleep environment, by the timing of sleep, severe depression, or by stress. Its consequences - sleepiness and impaired psychomotor performance - are similar to those of sleep deprivation.[6]
- Acute insomnia is the inability to consistently sleep well for a period of less than a month.[7]
- Chronic insomnia lasts for longer than a month. It can be caused by another disorder, or it can be a primary disorder. Its effects can vary according to its causes. They might include being unable to sleep, muscular fatigue, hallucinations, and/or mental fatigue; but people with chronic insomnia often show increased alertness. Some people that live with this disorder see things as if they are happening in slow motion, wherein moving objects seem to blend together. Can cause double vision.[6]
Patterns of insomnia
- Onset insomnia - difficulty falling asleep at the beginning of the night, often associated with anxiety disorders or the Delayed Sleep Phase Syndrome.
- Middle-of-the-Night Insomnia - Insomnia characterized by difficulty returning to sleep after awakening in the middle of the night or waking too early in the morning. Also referred to as nocturnal awakenings. Encompasses middle and terminal insomnia.
- Middle insomnia - waking during the middle of the night, difficulty maintaining sleep. Often associated with pain disorders or medical illness.
- Terminal (or late) insomnia - early morning waking. Often a characteristic of clinical depression.
Insomnia versus poor sleep quality
Poor sleep quality can occur as a result of sleep apnea or major depression. Poor sleep quality is caused by the individual not reaching stage 3 or delta sleep which has restorative properties. There are, however, people who are unable to achieve stage 3 sleep due to brain damage who lead perfectly normal lives.
Sleep apnea is a condition that occurs when a sleeping person's breathing is interrupted, thus interrupting the normal sleep cycle. With the obstructive form of the condition, some part of the sleeper's respiratory tract loses muscle tone and partially collapses. People with obstructive sleep apnea often do not remember awakening or having difficulty breathing, but they complain of excessive sleepiness during the day. Central sleep apnea interrupts the normal breathing stimulus of the central nervous system, and the individual must actually wake up to resume breathing. This form of apnea is often related to a cerebral vascular condition, congestive heart failure, and premature aging.
Major depression leads to alterations in the function of the hypothalamic-pituitary-adrenal axis, causing excessive release of cortisol which can lead to poor sleep quality.
Nocturnal polyuria, excessive nighttime urination, can be very disturbing to sleep.[8]
Some sleep disorders such as insomnia have been found to compromise glucose metabolism.[9]
Subjective insomnia
Some cases of insomnia are not really insomnia in the traditional sense. People experiencing sleep state misperception often sleep for normal durations, yet for some reason severely overestimate the time taken to fall asleep. In such cases, a person with sleep state misperception may believe they slept for only 4 hours while, paradoxically, sleeping a full 8 hours.
Signs and symptoms
A survey of 1.1 million residents in the United States conducted by the American Cancer Society found that those who reported sleeping about 7 hours per night had the lowest rates of mortality, whereas those who slept for fewer than 6 hours or more than 8 hours had higher mortality rates. Getting 8.5 or more hours of sleep per night increased the mortality rate by 15%. Severe insomnia - sleeping less than 3.5 hours in women and 4.5 hours in men - also led to a 15% increase in mortality. However, most of the increase in mortality from severe insomnia was discounted after controlling for comorbid disorders. After controlling for sleep duration and insomnia, use of sleeping pills was also found to be associated with an increased mortality rate.
The lowest mortality was seen in individuals who slept between six and a half and seven and a half hours per night. Even sleeping only 4.5 hours per night is associated with very little increase in mortality. Thus mild to moderate insomnia for most people is associated with increased longevity and severe insomnia is only associated with a very small effect on mortality.
As long as a patient refrains from using sleeping pills there is little to no increase in mortality associated with insomnia but there does appear to be an increase in longevity. This is reassuring for patients with insomnia in that despite the sometimes unpleasantness of insomnia, insomnia itself appears to be associated with increased longevity.
It is unclear why sleeping longer than 7.5 hours is associated with excess mortality.[10]
Causes
Insomnia can be caused by:
- Psychoactive drugs or stimulants, including certain medications, herbs, caffeine, nicotine, cocaine, amphetamines, methylphenidate, MDMA and modafinil
- Fluoroquinolone antibiotic drugs, see Fluoroquinolone toxicity, associated with more severe and chronic types of insomnia[11]
- Restless Legs Syndrome can cause insomnia due to the discomforting sensations felt and need to move the legs or other body parts to relieve these sensations. It is difficult if not impossible to fall asleep while moving.
- Pain[12] Any injury or condition that causes pain. Pain can preclude an individual from finding a comfortable position in which to fall asleep, and in addition can cause awakening if, during sleep, the person rolls over and puts pressure on the injured or painful area of the body.
- Hormone shifts such as those that precede menstruation and those during menopause
- Life problems like fear, stress, anxiety, emotional or mental tension, work problems, financial stress.
- Mental disorders such as bipolar disorder, clinical depression, generalized anxiety disorder, post traumatic stress disorder, schizophrenia, or obsessive compulsive disorder.
- Disturbances of the circadian rhythm, such as shift work and jet lag, can cause an inability to sleep at some times of the day and excessive sleepiness at other times of the day. Jet lag is seen in people who travel through multiple time zones, as the time relative to the rising and setting of the sun no longer coincides with the body's internal concept of it. The insomnia experienced by shift workers is also a circadian rhythm sleep disorder.
- Certain neurological disorders, brain lesions, or a history of traumatic brain injury
- Medical conditions such as hyperthyroidism and rheumatoid arthritis[13]
- Abuse of over-the counter or prescription sleep aids can produce rebound insomnia
- Poor sleep hygiene, e.g., noise
- Parasomnia, which includes a number of disruptive sleep events including nightmares, sleepwalking, night terrors, violent behavior while sleeping, and REM behavior disorder, in which a person moves his/her physical body in response to events within his/her dreams
- A rare genetic condition can cause a prion-based, permanent and eventually fatal form of insomnia called fatal familial insomnia.[14]
- Physical exercise. Exercise-induced insomnia is common in athletes, causing prolonged sleep onset latency.[15]
Sleep studies using polysomnography have suggested that people who have insomnia with sleep disruption have elevated nighttime levels of circulating cortisol and adrenocorticotropic hormone They also have an elevated metabolic rate, which does not occur in people who do not have insomnia but whose sleep is intentionally disrupted during a sleep study. Studies of brain metabolism using positron emission tomography (PET) scans indicate that people with insomnia have higher metabolic rates by night and by day. The question remains whether these changes are the causes or consequences of long-term insomnia.[13]
Insomnia can be common after the loss of a loved one, even years or decades after the death, if they have not gone through the grieving process. Overall, symptoms and the degree of their severity affect each individual differently depending on their mental health, physical condition, and attitude or personality.
A common misperception is that the amount of sleep required decreases as a person ages. The ability to sleep for long periods, rather than the need for sleep, appears to be lost as people get older. Some elderly insomniacs toss and turn in bed and occasionally fall off the bed at night, diminishing the amount of sleep they receive.[16]
Diagnosis
Specialists in sleep medicine are qualified to diagnose the many different sleep disorders. Patients with various disorders including delayed sleep phase syndrome are often mis-diagnosed with insomnia.
If a patient has trouble getting to sleep, but has normal sleep pattern once asleep, a circadian rhythm disorder is a likely cause.
Treatment for insomnia
In many cases, insomnia is caused by another disease, side effects from medications, or a psychological problem. It is important to identify or rule out medical and psychological causes before deciding on the treatment for the insomnia.[18] Attention to sleep hygiene is an important first line treatment strategy and should be tried before any pharmacological approach is considered.[19]
Non-pharmacological
Non-pharmacological strategies are superior to hypnotic medication for insomnia because tolerance develops to the hypnotic effects. In addition, dependence can develop with rebound withdrawal effects developing upon discontinuation. Hypnotic medication is therefore only recommended for short term use, especially in acute or chronic insomnia.[20] Non pharmacological strategies however, have long lasting improvements to insomnia and are recommended as a first line and long term strategy of managing insomnia. The strategies include attention to sleep hygiene, stimulus control, behavioral interventions, sleep-restriction therapy, paradoxical intention, patient education and relaxation therapy.[21]
EEG biofeedback has demonstrated effectiveness in the treatment of insomnia with improvements in duration as well as quality of sleep.[22]
Stimulus control therapy is a treatment for patients who have conditioned themselves to associate the bed, or sleep in general, with a negative response. As stimulus control therapy involves taking steps to control the sleep environment, it is sometimes referred interchangeably with the concept of sleep hygiene. Examples of such environmental modifications include using the bed for sleep or sex only, not for activities such as reading or watching television; waking up at the same time every morning, including on weekends; going to bed only when sleepy and when there is a high likelihood that sleep will occur; leaving the bed and beginning an activity in another location if sleep does not result in a reasonably brief period of time after getting into bed (commonly ~20 min); reducing the subjective effort and energy expended trying to fall asleep; avoiding exposure to bright light during nighttime hours, and eliminating daytime naps.
A component of stimulus control therapy is sleep restriction, a technique that aims to match the time spent in bed with actual time spent asleep. This technique involves maintaining a strict sleep-wake schedule, only sleeping at certain times of the day and for specific amounts of time to induce mild sleep deprivation. Complete treatment usually lasts up to 3 weeks and involves making oneself sleep for only a minimum amount of time that they are actually capable of on average, and then, if capable (i.e. when sleep efficiency improves), slowly increasing this amount (~15 min) by going to bed earlier as the body attempts to reset its internal sleep clock. Bright light therapy, which is often used to help early morning wakers reset their natural sleep cycle, can also be used with sleep restriction therapy to reinforce a new wake schedule. Although applying this technique with consistency is difficult, it can have a positive effect on insomnia in motivated patients.
Paradoxical intention is a cognitive reframing technique where the insomniac, instead of attempting to fall asleep at night, makes every effort to stay awake (i.e. essentially stops trying to fall asleep). One theory that may explain the effectiveness of this method is that by not voluntarily making oneself go to sleep, it relieves the performance anxiety that arises from the need or requirement to fall asleep, which is meant to be a passive act. This technique has been shown to reduce sleep effort and performance anxiety and also lower subjective assessment of sleep-onset latency and overestimation of the sleep deficit (a quality found in many insomniacs).[23]
Cognitive behavior therapy
A recent study found that cognitive behavior therapy is more effective than hypnotic medications in controlling insomnia.[24] In this therapy, patients are taught improved sleep habits and relieved of counter-productive assumptions about sleep. Common misconceptions and expectations that can be modified include: (1) unrealistic sleep expectations (e.g., I need to have 8 hours of sleep each night), (2) misconceptions about insomnia causes (e.g., I have a chemical imbalance causing my insomnia), (3) amplifying the consequences of insomnia (e.g., I cannot do anything after a bad night's sleep), and (4) performance anxiety after trying for so long to have a good night's sleep by controlling the sleep process. Numerous studies have reported positive outcomes of combining cognitive behavioral therapy treatment with treatments such as stimulus control and the relaxation therapies. Hypnotic medications are equally effective in the short term treatment of insomnia but their effects wear off over time due to tolerance. The effects of cognitive behavior therapy have sustained and lasting effects on treating insomnia long after therapy has been discontinued.[25][26] The addition of hypnotic medications with CBT adds no benefit in insomnia. The long lasting benefits of a course of CBT shows superiority over pharmacological hypnotic drugs. Even in the short term when compared to short term hypnotic medication such as zolpidem (Ambien), CBT still shows significant superiority. Thus CBT is recommended as a first line treatment for insomnia.[27]
Medications
Many insomniacs rely on sleeping tablets and other sedatives to get rest, with research showing that medications are prescribed to over 95% of insomniac cases.[28] Certain classes of sedatives such as benzodiazepines and newer nonbenzodiazepine drugs can also cause physical dependence which manifests in withdrawal symptoms if the drug is not carefully tapered down. The benzodiazepine and nonbenzodiazepine hypnotic medications also have a number of side effects such as day time fatigue, motor vehicle crashes, cognitive impairments and falls and fractures. Elderly people are more sensitive to these side effects.[29] The non-benzodiazepines zolpidem and zaleplon have not adequately demonstrated effectiveness in sleep maintenance. Some benzodiazepines have demonstrated effectiveness in sleep maintenance in the short-term but in the longer term is associated with tolerance and dependence. Drugs are in development which may prove more effective and safer than existing drugs for insomnia.[30]
In comparing the options, a systematic review found that benzodiazepines and nonbenzodiazepines have similar efficacy which was not significantly more than for antidepressants.[31] Benzodiazepines did not have a significant tendency for more adverse drug reactions.[31] Chronic users of hypnotic medications for insomnia do not have better sleep than chronic insomniacs who do not take medications. In fact, chronic users of hypnotic medications actually have more regular nighttime awakenings than insomniacs who do not take hypnotic medications.[32] A further review of the literature regarding benzodiazepine hypnotic as well as the nonbenzodiazepines concluded that these drugs caused an unjustifiable risk to the individual and to public health and lack evidence of long term effectiveness. The risks include dependence, accidents and other adverse effects. Gradual discontinuation of hypnotics in long term users leads to improved health without worsening of sleep. Preferably hypnotics should be prescribed for only a few days at the lowest effective dose and avoided altogether wherever possible in the elderly.[33]
Benzodiazepines
The most commonly used class of hypnotics prescribed for insomnia are the benzodiazepines. Benzodiazepines bind unselectively to the GABAA receptor.[31] These include drugs such as temazepam, flunitrazepam, triazolam, flurazepam, midazolam, nitrazepam and quazepam. These drugs can lead to tolerance, physical dependence and the benzodiazepine withdrawal syndrome upon discontinuation, especially after consistent usage over long periods of time. Benzodiazepines while inducing unconsciousness, actually worsen sleep as they promote light sleep whilst decreasing time spent in deep sleep such as REM sleep.[34] A further problem is with regular use of short acting sleep aids for insomnia, day time rebound anxiety can emerge.[35] Benzodiazepines can help to initiate sleep and increase sleep time but they also decrease deep sleep and increase light sleep. Although there is little evidence for benefit of benzodiazepines in insomnia and evidence of major harm prescriptions have continued to increase.[36] There is a general awareness that long-term use of benzodiazepines for insomnia in most people is inappropriate and that a gradual withdrawal is usually beneficial due to the adverse effects associated with the long-term use of benzodiazepines and is recommended whenever possible.[37][38]
Non-benzodiazepines
Nonbenzodiazepine sedative-hypnotic drugs, such as zolpidem, zaleplon, zopiclone and eszopiclone, are a newer classification of hypnotic medications. They work on the benzodiazepine site on the GABAA receptor complex similarly to the benzodiazepine class of drugs. Some but not all of the nonbenzodiazepines are selective for the α1 subunit on GABAA receptors which is responsible for inducing sleep and may therefore have a cleaner side effect profile than the older benzodiazepines. Zopiclone and eszopiclone like benzodiazepine drugs bind unselectively to α1, α2, α3 and α5 GABAA benzodiazepine receptors.[39] Zolpidem is more selective and zaleplon is highly selective for the α1 subunit, thus giving them an advantage over benzodiazepines in terms of sleep architecture and a reduction in side effects.[40][41] However, there are controversies over whether these non-benzodiazepine drugs are superior to benzodiazepines. These drugs appear to cause both psychological dependence and physical dependence though less than traditional benzodiazepines and can also cause the same memory and cognitive disturbances along with morning sedation.
Alcohol
Alcohol is often used as a form of self-treatment of insomnia to induce sleep. However, alcohol use to induce sleep can be a cause of insomnia. Long-term use of alcohol is associated with a decrease in NREM stage 3 and 4 sleep as well as suppression of REM sleep and REM sleep fragmentation. Frequent moving between sleep stages occurs, with awakenings due to headaches, polyuria, dehydration and diaphoresis. Glutamine rebound also plays a role as when someone is drinking, alcohol inhibits glutamine, one of the body's natural stimulants. When the person stops drinking, the body tries to make up for lost time by producing more glutamine than it needs. The increase in glutamine levels stimulates the brain while the drinker is trying to sleep, keeping them from reaching the deepest levels of sleep.[42] Stopping chronic alcohol use can also lead to severe insomnia with vivid dreams. During withdrawal REM sleep is typically exaggerated as part of a rebound effect.[43]
Opioids
Opioid medications such as hydrocodone, oxycodone, and morphine are used for insomnia which is associated with pain due to their analgesic properties and hypnotic effects. Opioids can fragment sleep and decrease REM and stage 2 sleep. By producing analgesia and sedation, opioids may be appropriate in carefully selected patients with pain-associated insomnia.[12]
Antidepressants
Some antidepressants such as amitriptyline, doxepin, mirtazapine, and trazodone can often have a very strong sedative effect, and are prescribed off label to treat insomnia.[44] The major drawback of these drugs is that they have properties which can lead to many side effects, for example; amitriptyline and doxepin both have antihistaminergic, anticholinergic and antiadrenergic properties which contribute to their side effect profile, while mirtazapines side effects are primarily antihistaminergic, and trazadones side effects are primarily antiadrenergic. Some also alter sleep architecture. As with benzodiazepines, the use of antidepressants in the treatment of insomnia can lead to withdrawal effects; withdrawal may induce rebound insomnia.
Mirtazapine is known to decrease sleep latency, promoting sleep efficiency and increasing the total amount of sleeping time in patients suffering from both depression and insomnia.[45][46]
Melatonin and melatonin agonists
The hormone and supplement melatonin is effective in several types of insomnia. Melatonin has demonstrated effectiveness equivalent to the prescription sleeping tablet zopiclone in inducing sleep and regulating the sleep/waking cycle.[47] One particular benefit of melatonin is that it can treat insomnia without altering the sleep pattern which is altered by many prescription sleeping tablets. Another benefit is it does not impair performance related skills.[48][49]
Melatonin agonists, including ramelteon (Rozerem) and tasimelteon, seem to lack the potential for misuse and dependence. This class of drugs has a relatively mild side effect profile and lower likelihood of causing morning sedation. While these drugs show good effects for the treatment of insomnia due to jet lag,[50] the results for other forms of insomnia are less promising.[51]
Natural substances such as 5-HTP and L-Tryptophan have been said to fortify the serotonin-melatonin pathway and aid people with various sleep disorders including insomnia.[52]
Antihistamines
The antihistamine diphenhydramine is widely used in nonprescription sleep aids such as Benadryl. The antihistamine doxylamine is used in nonprescription sleep aids such as Unisom (USA) and Unisom 2 (Canada). In some countries, including Australia, it is marketed under the names Restavit and Dozile. It is the most effective over-the-counter sedative currently available in the United States, and is more sedating than some prescription hypnotics.[53]
While the two drugs mentioned above are available over the counter in most countries, the effectiveness of these agents may decrease over time and the incidence of next-day sedation is higher than for most of the newer prescription drugs. Anticholinergic side effects may also be a draw back of these particular drugs. Dependence does not seem to be an issue with this class of drugs.
Cyproheptadine is a useful alternative to benzodiazepine hypnotics in the treatment of insomnia. Cyproheptadine may be superior to benzodiazepines in the treatment of insomnia because cyproheptadine enhances sleep quality and quantity whereas benzodiazepines tend to decrease sleep quality.[54]
Atypical antipsychotics
Low doses of certain atypical antipsychotics such as quetiapine, olanzapine and risperidone are also prescribed for their sedative effect but the danger of neurological, metabolic and cognitive side effects make these drugs a poor choice to treat insomnia. Over time, quetiapine may lose its effectiveness as a sedative. The ability of quetiapine to produce sedation is determined by the dosage. Higher doses (300 mg - 900 mg) are usually taken for its use as an antipsychotic, while lower doses (25 mg - 200 mg) have a marked sedative effect, e.g. if a patient takes 300 mg, he/she will more likely benefit from the drug's antipsychotic effects, but if the dose is brought down to 100 mg, it will leave the patient feeling more sedated than at 300 mg, because it primarily works as a sedative at lower doses.
Eplivanserin is an investigational drug with a mechanism similar to these antipsychotics, but probably with less side effects.
Other substances
Some insomniacs use herbs such as valerian, chamomile, lavender, hops, and passion-flower. Valerian has undergone multiple studies and appears to be modestly effective.[55][56][57].
Insomnia may be a symptom of magnesium deficiency, or low magnesium levels, but this has not yet been proven. A healthy diet containing magnesium can help to improve sleep in individuals without an adequate intake of magnesium.[58]

Epidemiology
The National Sleep Foundation's 2002 Sleep in America poll showed that 58% of adults in the U.S. experienced symptoms of insomnia a few nights a week or more.[59] Although insomnia was the most common sleep problem among about one half of older adults (48%), they were less likely to experience frequent symptoms of insomnia than their younger counterparts (45% vs. 62%), and their symptoms were more likely to be associated with medical conditions, according to the 2003 poll of adults between the ages of 55 and 84.[59]
See also
- Sleep state misperception
- Somniphobia
- Fatal familial insomnia
- Sleep deprivation
- Delayed sleep phase syndrome
- Actigraphy
- Thai Ngoc, Vietnamese insomniac, claimed to be awake for 33 years
- Al Herpin, American insomniac, known as the "Man Who Never Slept"
References
- ↑ Hirshkowitz, Max (2004). "Chapter 10, Neuropsychiatric Aspects of Sleep and Sleep Disorders (pp 315-340)". In Stuart C. Yudofsky and Robert E. Hales, editors (Google Books preview includes entire chapter 10). Essentials of neuropsychiatry and clinical neurosciences (4 ed.). Arlington, Virginia, USA: American Psychiatric Publishing. ISBN 9781585620050. http://books.google.no/books?id=XKhu7yb3QtsC&pg=PA315&lpg=PA315&dq=%22Max+Hirshkowitz%22&source=bl&ots=Rt5ZMiMbxt&sig=7upt8PudAdiA5f9kk5KGsrfaMQU&hl=no&ei=y-0bS7vFKtTP-QabhdTaDw&sa=X&oi=book_result&ct=result&resnum=3&ved=0CBIQ6AEwAjgK#v=onepage&q=%22Max%20Hirshkowitz%22&f=false. Retrieved 2009-12-06. "...insomnia is a symptom. It is neither a disease nor a specific condition. (from p. 322)"
- ↑ "WHO technical meeting on sleep and health" (pdf). http://www.euro.who.int/document/E84683_1.pdf. Retrieved 2009-01-25. "Dyssomnias" (pdf). WHO. pp. 7–11. http://www.who.int/selection_medicines/committees/expert/17/application/Section24_GAD.pdf. Retrieved 2009-01-25.
- ↑ Morin, Charles M. (2000). "The Nature of Insomnia and the Need to Refine Our Diagnostic Criteria" (Editorial). Psychosomatic Medicine 62 (4): 62:483–485. PMID 10949092. http://www.psychosomaticmedicine.org/cgi/content/full/62/4/483. Retrieved 2010-01-07.
- ↑ "Brain Basics: Understanding Sleep: National Institute of Neurological Disorders and Stroke (NINDS)". http://www.ninds.nih.gov/disorders/brain_basics/understanding_sleep.htm. Retrieved 2007-12-16.
- ↑ "Several Sleep Disorders Reflect Gender Differences". http://pn.psychiatryonline.org/cgi/content/full/42/10/40. Retrieved 2008-09-05.
- ↑ 6.0 6.1 Roth, Thomas; Timothy Roehrs (2004-02-25). "Insomnia: Epidemiology, characteristics, and consequences". Clinical Cornerstone 5 (3): 5–15. doi:10.1016/S1098-3597(03)90031-7. PMID 14626537.
- ↑ "Insomnia - sleeplessness, chronic insomnia, acute insomnia, mental ...". driectoryM articles. http://articles.directorym.com/Insomnia-a352.html. Retrieved 2008-04-29.
- ↑ Sleep issues in Parkinson’s disease. Neurology. 2005. pp. 64; S12–20. http://www.neurology.org/cgi/content/full/64/12_suppl_3/S12. Retrieved June 2007.
- ↑ Keckeis M, Lattova Z, Maurovich-Horvat E, Beitinger PA, Birkmann S, Lauer CJ, Wetter TC, Wilde-Frenz J, Pollmächer T. (2010). "Impaired glucose tolerance in sleep disorders.". PloS 1. 3 (5): 9444. doi:10.1371/journal.pone.0009444. PMID 20209158.
- ↑ Kripke DF, Garfinkel L, Wingard DL, Klauber MR, Marler MR (February 2002). "Mortality associated with sleep duration and insomnia". Arch. Gen. Psychiatry 59 (2): 131–6. doi:10.1001/archpsyc.59.2.131. PMID 11825133. http://archpsyc.ama-assn.org/cgi/content/full/59/2/131.
- ↑ Lawrence KR, Adra M, Keir C (June 2006). "Hypoglycemia-induced anoxic brain injury possibly associated with levofloxacin". J. Infect. 52 (6): e177–80. doi:10.1016/j.jinf.2005.08.024. PMID 16269178.
- ↑ 12.0 12.1 Ramakrishnan, K.; Scheid, DC. (Aug 2007). "Treatment options for insomnia.". Am Fam Physician 76 (4): 517–26. PMID 17853625. http://www.aafp.org/afp/2007/0815/p517.html.
- ↑ 13.0 13.1 Mendelson WB (2008). "New Research on Insomnia: Sleep Disorders May Precede or Exacerbate Psychiatric Conditions". Psychiatric Times 25 (7). http://www.psychiatrictimes.com/insomnia/article/10168/1163082.
- ↑ Schenkein J, Montagna P (2006). "Self management of fatal familial insomnia. Part 1: what is FFI?". MedGenMed : Medscape general medicine 8 (3): 65. PMID 17406188.
- ↑ The epidemiological survey of exercise-induced insomnia in chinese athletes Youqi Shi, Zhihong Zhou, Ke Ning, Jianhong LIU. Athens 2004: Pre-olympic Congress.
- ↑ American Family Physician: Chronic Insomnia: A Practical Review
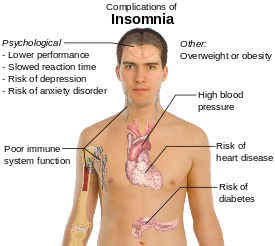
- ↑ Mayo Clinic > Insomnia > Complications By Mayo Clinic staff. Retrieved on May 5, 2009
- ↑ Wortelboer U, Cohrs S, Rodenbeck A, Rüther E (2002). "Tolerability of hypnosedatives in older patients". Drugs Aging 19 (7): 529–39. doi:10.2165/00002512-200219070-00006. PMID 12182689.
- ↑ Flamer HE (June 1995). "Sleep problems". Med. J. Aust. 162 (11): 603–7. PMID 7791648.
- ↑ National Prescribing Service (2009). "Addresing hypnotic medicines use in primary care". NPS News, Vol 67. Available at http://www.nps.org.au/health_professionals/publications/nps_news/current/nps_news_67
- ↑ Kirkwood CK (1999). "Management of insomnia". J Am Pharm Assoc 39 (5): 688–96; quiz 713–4. PMID 10533351.
- ↑ Lake, James A. (31 October 2006). Textbook of Integrative Mental Health Care. Thieme Medical Publishers. p. 313. ISBN 1-58890-299-4. http://books.google.com/?id=Bt5euqMwbpYC&pg=PA313.
- ↑ Kierlin L (2008). "Sleeping without a pill: nonpharmacologic treatments for insomnia". J Psychiatr Pract 14 (6): 403–7. doi:10.1097/01.pra.0000341896.73926.6c. PMID 19057243.
- ↑ Cognitive behavior therapy and pharmacotherapy for insomnia: a randomized controlled trial and direct comparison, http://www.ncbi.nlm.nih.gov/pubmed/15451764?dopt=Abstract
- ↑ Jacobs, Gregg; Edward F. Pace-Schott, Robert Stickgold, Michael W. Otto (September 27, 2004). "Cognitive Behavior Therapy and Pharmacotherapy for Insomnia: A Randomized Controlled Trial and Direct Comparison". Archives of Internal Medicine 164 (17): 1888–1896. doi:10.1001/archinte.164.17.1888. PMID 15451764. http://archinte.ama-assn.org/cgi/content/full/164/17/1888?ijkey=6a2af558a671b089d7c77db5fc5f53a450fd1cda.
- ↑ Morin, C. M.; Colecchi, C; Stone, J; Sood, R; Brink, D (1999). "Behavioral and Pharmacological Therapies for Late-Life Insomnia: A Randomized Controlled Trial". JAMA the Journal of the American Medical Association 281 (11): 991. doi:10.1001/jama.281.11.991. PMID 10086433. http://jama.ama-assn.org/cgi/content/full/281/11/991.
- ↑ KARL E. MILLER, M.D. (July 2005). "Cognitive Behavior Therapy vs. Pharmacotherapy for Insomnia". American Family Physician. http://www.aafp.org/afp/20050715/tips/7.html.
- ↑ Harrison C, Britt H (2009). "Insomnia". Australian Family Physician, 32:283. Available at http://www.racgp.org.au/afp/200905/200905beach.pdf and http://www.nps.org.au/news_and_media/media_releases/repository/New_clinical_program_addresses
- ↑ Glass J, Lanctôt KL, Herrmann N, Sproule BA, Busto UE (November 2005). "Sedative hypnotics in older people with insomnia: meta-analysis of risks and benefits". BMJ 331 (7526): 1169. doi:10.1136/bmj.38623.768588.47. PMID 16284208. PMC 1285093. http://www.bmj.com/cgi/content/full/331/7526/1169.
- ↑ Rosenberg, RP. (Jan-Mar 2006). "Sleep maintenance insomnia: strengths and weaknesses of current pharmacologic therapies.". Ann Clin Psychiatry 18 (1): 49–56. doi:10.1080/10401230500464711. PMID 16517453.
- ↑ 31.0 31.1 31.2 Buscemi N, Vandermeer B, Friesen C, Bialy L, Tubman M, Ospina M, Klassen TP, Witmans M. (September 2007). "The efficacy and safety of drug treatments for chronic insomnia in adults: a meta-analysis of RCTs". J Gen Intern Med 22 (9): 1335–1350. doi:10.1007/s11606-007-0251-z. PMID 17619935.
- ↑ Ohayon MM, Caulet M (May 1995). "Insomnia and psychotropic drug consumption". Prog. Neuropsychopharmacol. Biol. Psychiatry 19 (3): 421–31. doi:10.1016/0278-5846(94)00023-B. PMID 7624493. http://linkinghub.elsevier.com/retrieve/pii/027858469400023B.
- ↑ "What's wrong with prescribing hypnotics?". Drug Ther Bull 42 (12): 89–93. December 2004. doi:10.1136/dtb.2004.421289. PMID 15587763. http://www.nelm.nhs.uk/en/NeLM-Area/Evidence/Drug-Class-Focused-Reviews/498264/.
- ↑ Tsoi, Wf (March 1991). "Insomnia: drug treatment.". Annals of the Academy of Medicine, Singapore 20 (2): 269–72. ISSN 0304-4602. PMID 1679317.
- ↑ Montplaisir J (August 2000). "Treatment of primary insomnia" (PDF). CMAJ 163 (4): 389–91. PMID 10976252. PMC 80369. http://www.pubmedcentral.nih.gov/articlerender.fcgi?tool=pubmed&pubmedid=10976252.
- ↑ D. Maiuro PhD, Roland (13 December 2009). Handbook of Integrative Clinical Psychology, Psychiatry, and Behavioral Medicine: Perspectives, Practices, and Research. Springer Publishing Company. pp. 128–130. ISBN 0-8261-1094-0. http://books.google.com/?id=4Tkdm1vRFbUC.
- ↑ Lader, Malcolm Harold; P. Cardinali, Daniel; R. Pandi-Perumal, S. (22 March 2006). Sleep and sleep disorders: a neuropsychopharmacological approach. Georgetown, Tex.: Landes Bioscience/Eurekah.com. p. 127. ISBN 0-387-27681-5.
- ↑ Authier, N.; Boucher, A.; Lamaison, D.; Llorca, PM.; Descotes, J.; Eschalier, A. (2009). "Second Meeting of the French CEIP (Centres d'Evaluation et d'Information sur la Pharmacodépendance). Part II: Benzodiazepine Withdrawal.". Therapie 64 (6): 365–370. doi:10.2515/therapie/2009051. PMID 20025839.
- ↑ WHO (2006). "World Health Organisation - Assessment of Zopiclone" (PDF). who.int. http://www.who.int/medicines/areas/quality_safety/4.6ZopicloneCritReview.pdf.
- ↑ Rowlett JK, Woolverton WL (November 1996). "Assessment of benzodiazepine receptor heterogeneity in vivo: apparent pA2 and pKB analyses from behavioral studies" (PDF). Psychopharmacology (Berl.) 128 (1): 1–16. doi:10.1007/s002130050103. PMID 8944400. http://www.springerlink.com/content/xeu44evyanvw1n65/fulltext.pdf.
- ↑ Noguchi H; Kitazumi K, Mori M, Shiba T. (March 2004). "Electroencephalographic properties of zaleplon, a non-benzodiazepine sedative/hypnotic, in rats" (pdf). J Pharmacol Sci. 94 (3): 246–51. doi:10.1254/jphs.94.246. PMID 15037809. http://www.jstage.jst.go.jp/article/jphs/94/3/246/_pdf.
- ↑ http://health.howstuffworks.com/hangover5.htm
- ↑ Lee-chiong, Teofilo (24 April 2008). Sleep Medicine: Essentials and Review. Oxford University Press, USA. p. 105. ISBN 0-19-530659-7. http://books.google.com/?id=s1F_DEbRNMcC&pg=PT105.
- ↑ Bertschy G, Ragama-Pardos E, Muscionico M, et al (January 2005). "Trazodone addition for insomnia in venlafaxine-treated, depressed inpatients: a semi-naturalistic study". Pharmacol. Res. 51 (1): 79–84. doi:10.1016/j.phrs.2004.06.007. PMID 15519538.
- ↑ Winokur A, DeMartinis NA 3rd, McNally DP, Gary EM, Cormier JL, Gary KA. , et al (August pmid=14658972 2003). "Comparative effects of mirtazapine and fluoxetine on sleep physiology measures in patients with major depression and insomnia". J Clin Psychiatry.
- ↑ Schittecatte M, Dumont F, Machowski R, Cornil C, Lavergne F, Wilmotte J , et al (2002). "Effects of mirtazapine on sleep polygraphic variables in major depression". Neuropsychobiology year=2002 46 (4): 197–201. doi:10.1159/000067812. PMID 12566938.
- ↑ Paul MA, Gray G, Sardana TM, Pigeau RA (May 2004). "Melatonin and zopiclone as facilitators of early circadian sleep in operational air transport crews". Aviat Space Environ Med 75 (5): 439–43. PMID 15152897.
- ↑ Paul MA, Gray G, Kenny G, Pigeau RA (December 2003). "Impact of melatonin, zaleplon, zopiclone, and temazepam on psychomotor performance". Aviat Space Environ Med 74 (12): 1263–70. PMID 14692469.
- ↑ Zhdanova IV, Tucci V (May 2003). "Melatonin, Circadian Rhythms, and Sleep" (– Scholar search). Curr Treat Options Neurol 5 (3): 225–229. doi:10.1007/s11940-003-0013-0. PMID 12670411. http://www.treatment-options.com/1092-8480/5/225.
- ↑ Rajaratnam, SMW; Polymeropoulos MH, Fisher DM, Roth T, Scott C, Birznieks G, Klerman EB (2 December 2008). "Melatonin agonist tasimelteon (VEC-162) for transient insomnia after sleep-time shift: two randomised controlled multicentre trials". Lancet 373 (9662): 482. doi:10.1016/S0140-6736(08)61812-7. PMID 19054552.
- ↑ Zammit G, Erman M, Wang-Weigand S, Sainati S, Zhang J, Roth T (August 2007). "Evaluation of the efficacy and safety of ramelteon in subjects with chronic insomnia". J Clin Sleep Med 3 (5): 495–504. PMID 17803013.
- ↑ Morton Walker, DPM - The Restoration of L-Tryptophan with Its Numerous Physiological Benefits
- ↑ DrugBank: DB00366 (Doxylamine)
- ↑ Tokunaga S; Takeda Y, Shinomiya K, Hirase M, Kamei C. (February 2007). "Effects of some H1-antagonists on the sleep-wake cycle in sleep-disturbed rats" (pdf). J Pharmacol Sci. 103 (2): 201–6. doi:10.1254/jphs.FP0061173. PMID 17287588. http://www.jstage.jst.go.jp/article/jphs/103/2/201/_pdf.
- ↑ Donath F, Quispe S, Diefenbach K, Maurer A, Fietze I, Roots I (2000). "Critical evaluation of the effect of valerian extract on sleep structure and sleep quality". Pharmacopsychiatry 33 (2): 47–53. doi:10.1055/s-2000-7972. PMID 10761819.
- ↑ Morin CM, Koetter U, Bastien C, Ware JC, Wooten V (2005). "Valerian-hops combination and diphenhydramine for treating insomnia: a randomized placebo-controlled clinical trial". Sleep 28 (11): 1465–71. PMID 16335333.
- ↑ Meolie AL, Rosen C, Kristo D, et al (2005). "Oral nonprescription treatment for insomnia: an evaluation of products with limited evidence". Journal of clinical sleep medicine : JCSM : official publication of the American Academy of Sleep Medicine 1 (2): 173–87. PMID 17561634.
- ↑ Hornyak M, Voderholzer U, Hohagen F, Berger M, Riemann D (1998). "Magnesium therapy for periodic leg movements-related insomnia and restless legs syndrome: an open pilot study". Sleep 21 (5): 501–5. PMID 9703590.
- ↑ 59.0 59.1 "2002 Sleep in America Poll". National Sleep Foundation. http://www.sleepfoundation.org/site/c.huIXKjM0IxF/b.2417355/k.143E/2002_Sleep_in_America_Poll.htm. Retrieved 2008-08-13.
|
|||||||||||||||||||||||||||||||||||||||
|
||||||||||||||||||||||||||||||